Part 1: Group Sequential and Adaptive Designs
GKM
December 12, 2024
Group Sequential Designs: Basic Theory
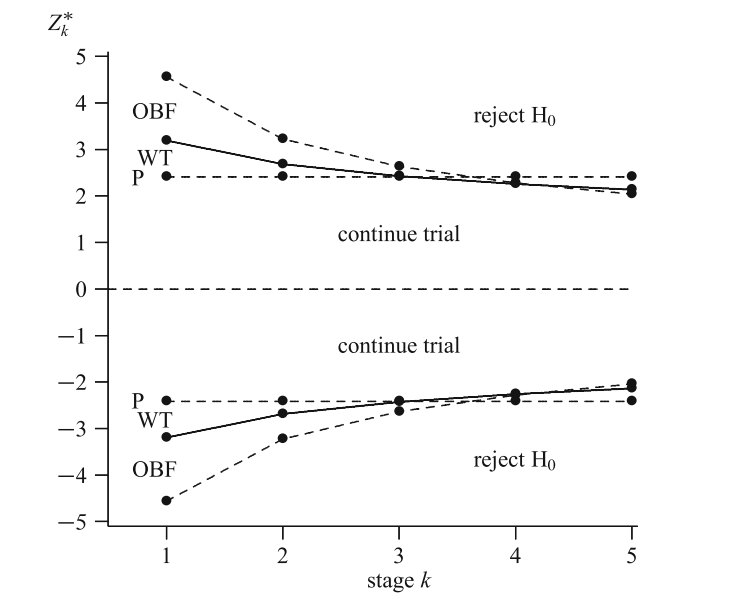
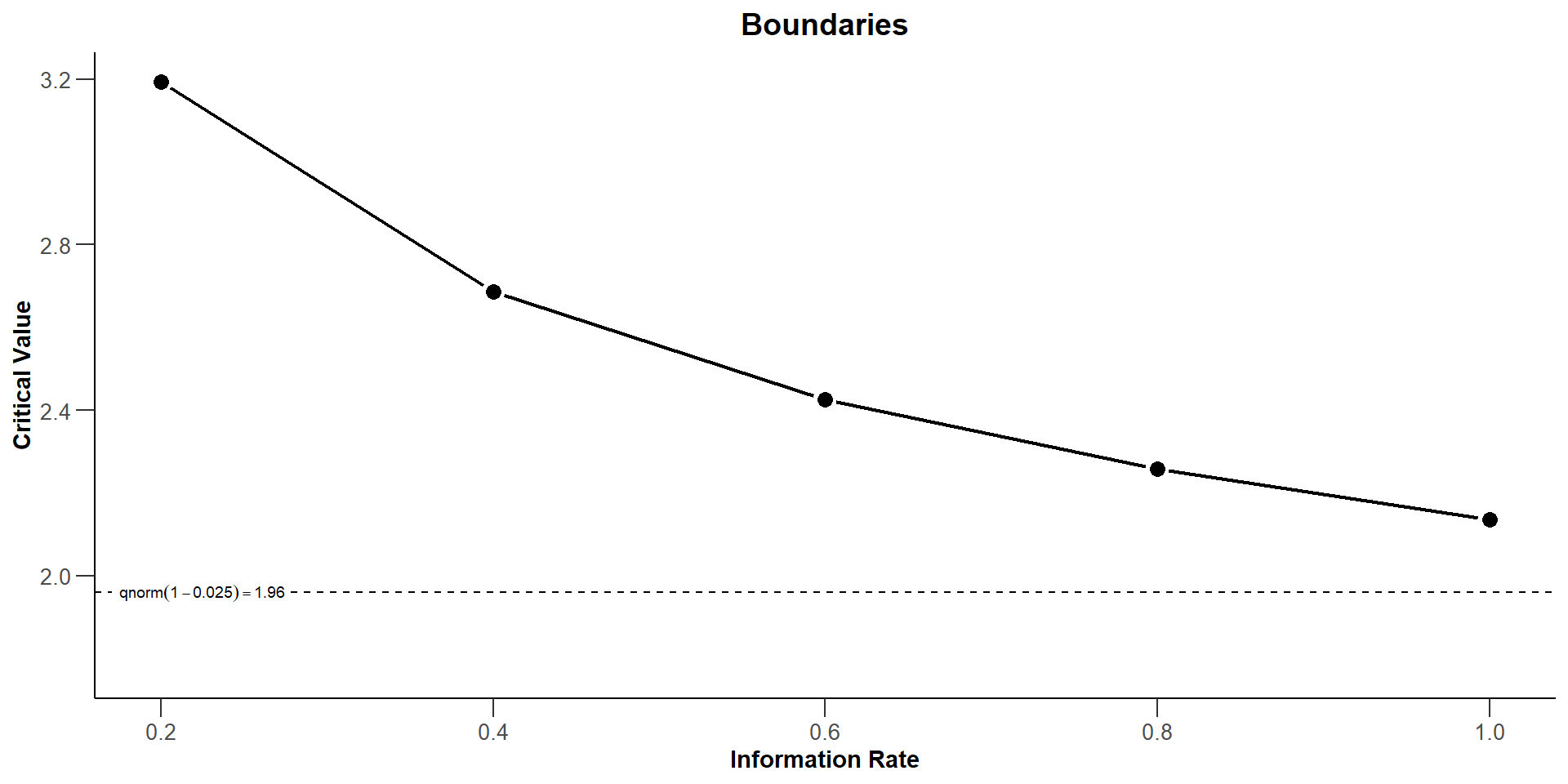
Pocock and O’Brien and Fleming design
Wang and Tsiatis \(\Delta\)-class \(u_k = k^{\Delta-0.5}\). O’Brien and Fleming: \(\Delta\) = 0; Pocock: \(\Delta\) = 0.5
How this is done with rpact
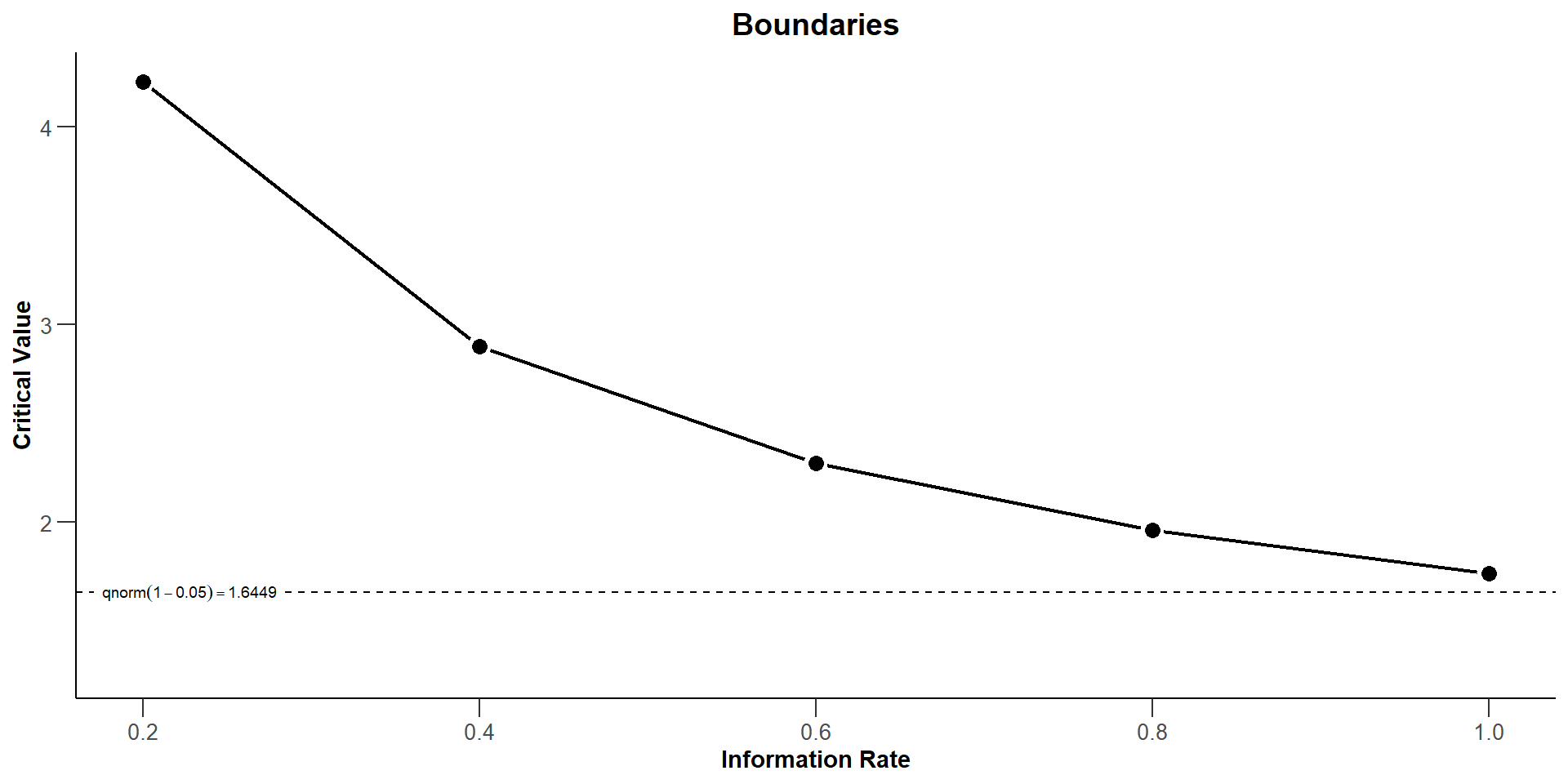
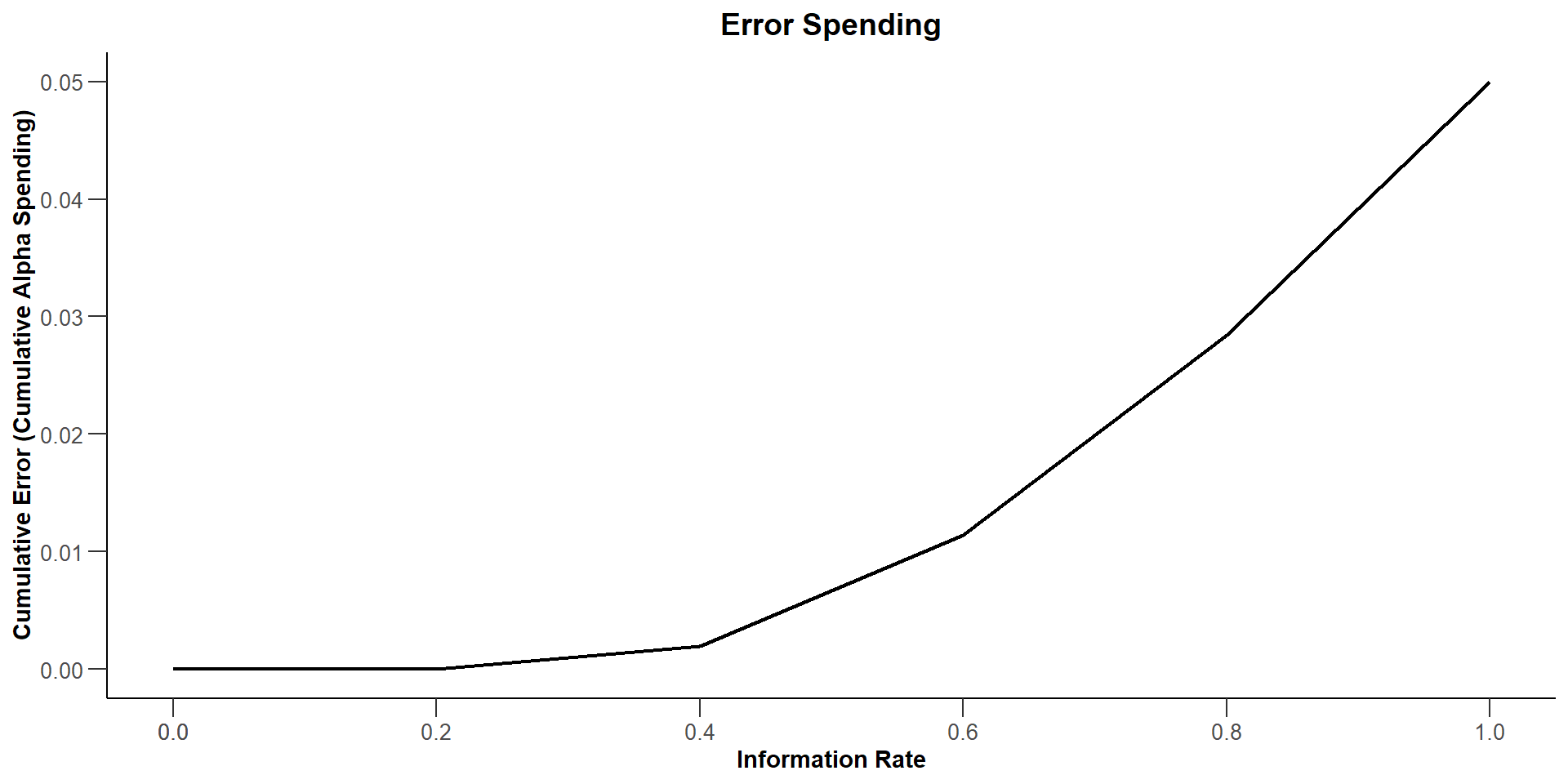
The Use Function Approach
Examples of \(\alpha\)-spending functions
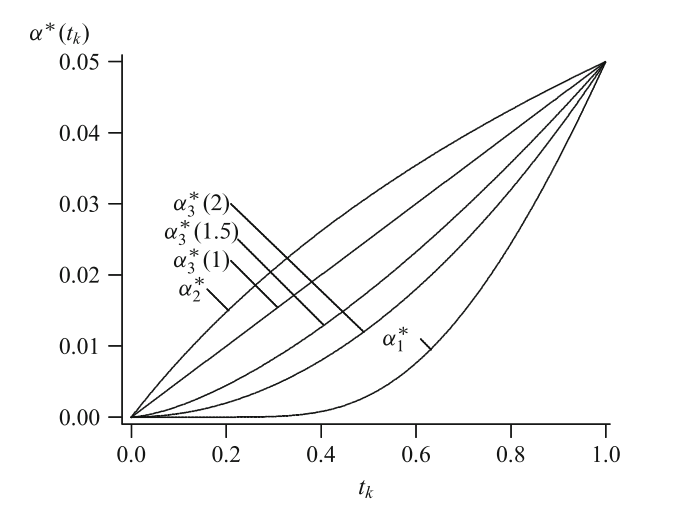
Examples of \(\alpha\)-spending functions. \(\alpha_1^*\) and \(\alpha_2^*\) approximate O’Brien and Fleming’s and Pocock’s design, respectively. \(\alpha_3^*(\varrho)\) is plotted for \(\varrho = 1.0\), \(1.5\), and \(2.0\); \(\alpha = 0.05\).
With rpact
The Combination Test (Bauer ’89, Bauer & Köhne ’94)
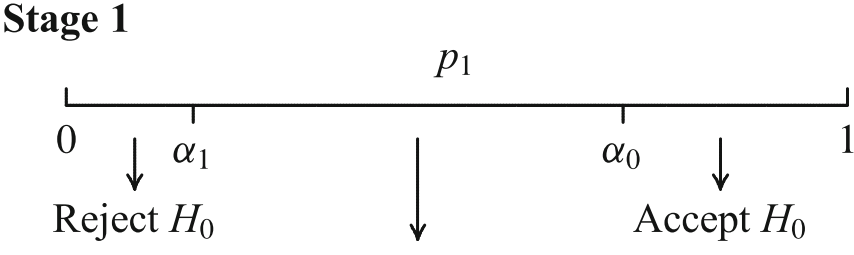

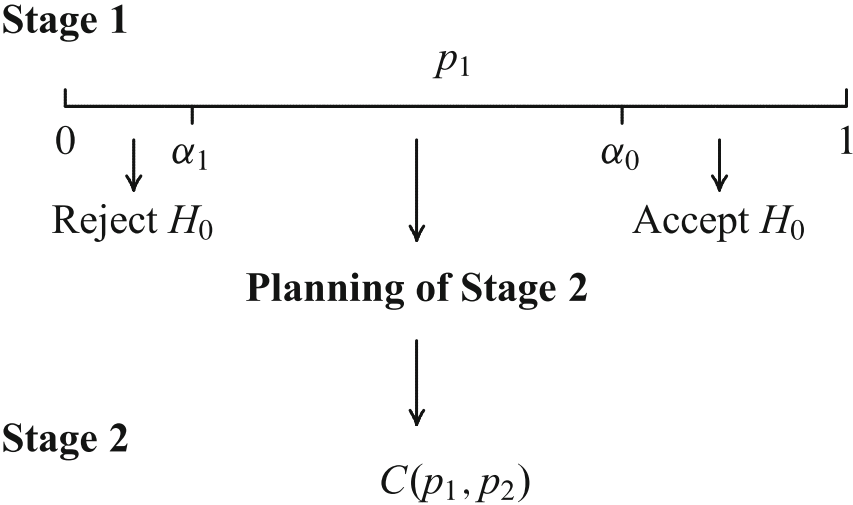

Stopping boundaries and combination functions have to be laid down a priori!
Seamless Phase II/III Trials: Treatment Arm Selection
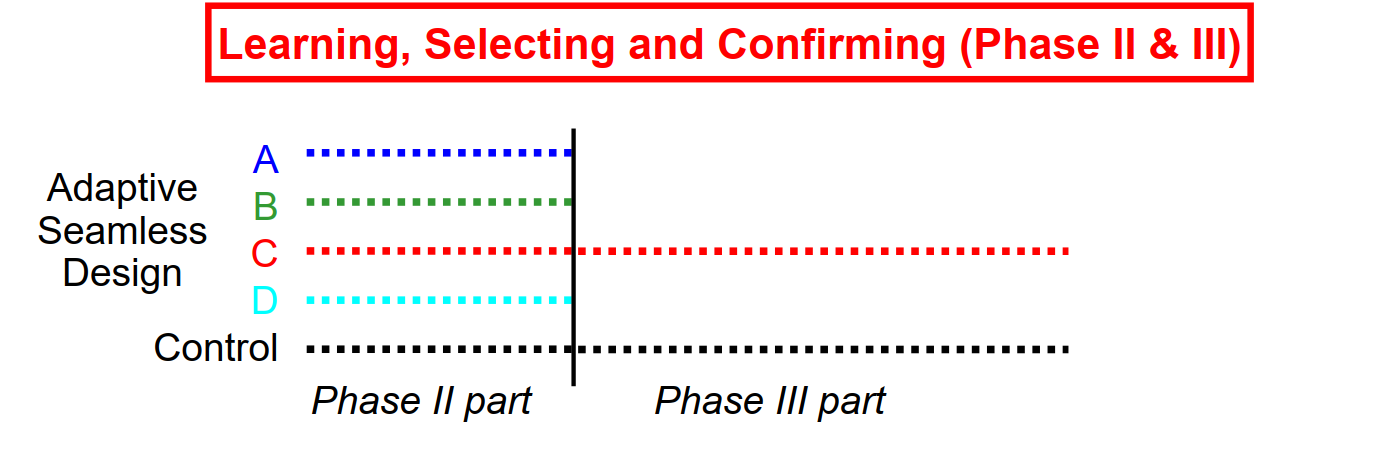 - Conduct phase II trial as internal part of a combined trial - Plan phase III trial based on data from phase II part - Conduct phase III trial as internal part of the same trial - Demonstrate efficacy with data from phase III + II part
- Conduct phase II trial as internal part of a combined trial - Plan phase III trial based on data from phase II part - Conduct phase III trial as internal part of the same trial - Demonstrate efficacy with data from phase III + II part
Enrichment: Phase 2/3 Study in HER2- Early Stage BC
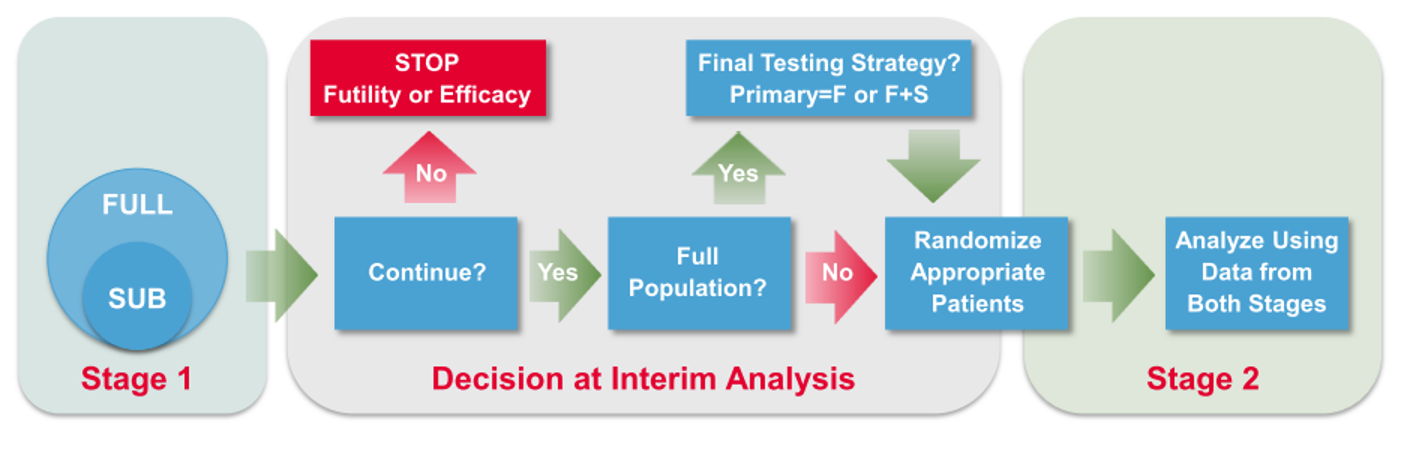
- Stage 1 objective
- Stop for futility/efficacy
- To continue with HER2- (Full) population – Broad Label (F) or Enhanced Label (F+S)
- To confirm greater benefit in TNBC Subpopulation – Restricted Label (S)
- To adjust the sample size
- Stage 2 data and the relevant groups from Stage 1 data combined
Book reference: Wassmer and Brannath (2016)

See also:
Twenty-five years of confirmatory adaptive designs: opportunities and pitfalls P. Bauer, F. Bretz, V. Dragalin, F. König, and G. Wassmer. Featured Article in Statistics in Medicine 35, 325-347, 2016. http://dx.doi.org/10.1002/sim.6472 (Open Access)
With invited discussion by Hung, Wang and Lawrence; Mehta and Liu; Vollmar; Maurer
The Future